




2% of the UK population have a diagnosed allergy and many of those will be carrying an adrenalin auto-injector. We trust them, we know these little devices save lives and they give us some security that we have instant access to the drugs that will hopefully reverse an anaphylactic reaction and give time for emergency services to arrive.
But how many of the adrenaline carrying public have the same depth of skin, fat and muscle in their thigh?
Directions of where to inject can vary but you can watch video’s on the websites of the auto-injector you use. It’s usually suggested to inject the outer thigh about a third of the way down from your hip to knee.
Does it matter where in the thigh adrenaline is administered? Knowing that human beings all come in very different shapes and sizes, especially women, suggests that possibly this might vary considerably from person to person.
Does it matter which adrenalin auto-injector I have and where to inject?
The needle length for both EpiPen and Jext is approximately 15mm. For the Emmerade the needle length is quite a bit longer at 25mm. How significant could this length be? and is 25mm even enough in some cases?
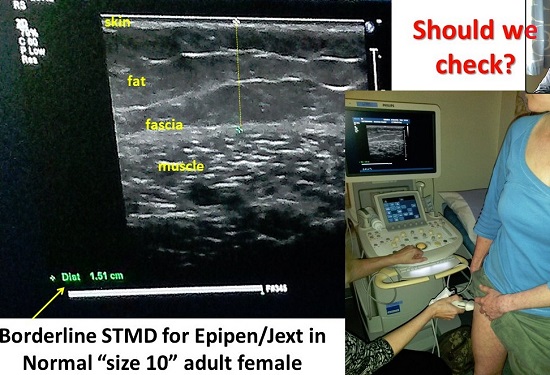
Take the image above of my skinny thighs being ultrasounded. I wanted to check that my adrenaline auto-injector would work as I’ve use one on a number of occasions and never actually felt like anything was happening.
Having spoken to other people and heard how they felt, you should experience a massive rush of adrenaline, literally. You might feel dizzy, light headed, get a head ache, but you should most definitely feel like something is happening. I have always felt nothing at all, and as if the reaction was just carrying on. Not encouraging at all.
Mine are fairly lean size 10 thighs and I do try to keep fairly fit, walking, cycling and yoga. So would my fat to muscle ratio put my mind at rest? You can see above that the depth scanned showed that it would just about be suitable for either EpiPen, Jext or Emerade but the distance on my legs was borderline with only a few mil to spare. However at the top of the thigh where some instructions and videos suggest injecting, there is only JUST about enough depth for the adrenalin to penetrate through the muscle. If the layer of fat to muscle is too thick this may mean adrenaline will not get into the body fast enough and whilst some may get into your system, you may not get the full dose. Adrenaline needs to be injected straight into muscle to work effectively.
I now have an Emerade auto-injector as I felt that the ultrasound was a little worrying. My weight can vary from month to month, this ultrasound was done when I was fairly skinny and when I previously used the adrenaline I know I was heavier by about a dress size. Could this have been enough to mean the adrenaline didn’t get into my muscle properly?
If you are injecting through clothing, as is normal with the guidelines for using auto-injectors you would need to add a millimetre or so to that depth. If you were wearing thick denim jeans perhaps even more.
The adrenaline auto-injector review
The following statement is from The European Medicines Agency website who are currently reviewing all adrenaline auto-injectors:
“The European Medicines Agency (EMA) are currently reviewing the adrenaline auto-injectors approved in the UK. Adrenaline auto-injectors need to deliver adrenaline into the muscle, the UK review concluded that there is no robust evidence that this is the case for all patients.
Depending on individual factors such as skin-to-muscle depth, adrenaline may instead be injected under the skin (but not into a muscle), which may result in a different absorption profile (uptake of the medicine by the body).
The European Medicines Agency will now review the available data on the delivery of adrenaline from auto-injectors and on whether the product information contains clear and detailed instructions for appropriate use, and issue an opinion on the marketing authorisations of these medicines across the European Union (EU).
It is important that patients continue to carry an adrenaline auto-injector with which they are familiar, so that they can use it confidently in an emergency if needed. Patients who suffer an anaphylactic reaction should use their injector as prescribed and seek emergency medical assistance straight away.”
Michelle Berridale-Johnson of Foods Matter debates this very subject, suggesting that since these injectors were designed for the lean thigh muscles of fit army personnel they may very well not be quite fit for purpose for the varying sizes of the general population. You can read more in ‘The needle debate in anaphylaxis treatment’.
Don’t panic!
The Anaphylaxis Campaign website has some information about this review available too and if you are at all in doubt please call their helpline on 01252 542029, email info@anaphylaxis.org.uk or speak to your doctor. What is important is that you don’t panic, and please continue to carry your adrenaline with you at all times. My advice, if you are worried would be to take the details of the review to your doctor and ask for an ultrasound to find your optimal ‘spot’ or area that will be effective for your pen. They should provide this examination for free and it will only take a matter of minutes. Ultrasound equipment is available all across the country so there should be no excuse for not finding an appointment.
You can also investigate getting an Emerade pen which has a longer needle.
Some initial studies show that most men should be fine with any injector, but some women may not so make sure you are not one of those. A few recent deaths of young slim women who have died of anaphylaxis despite being injected correctly with more than one adrenaline auto-injector. Could it have been that their injector just couldn’t reach their muscle?
Please, please don’t panic about this. The review is great news because none of us want to feel we are just carrying around a placebo. Adrenaline can save lives but only if is injected into muscle correctly. If it has no chance of ever reaching your muscle it’s useless! What my ultrasound showed above is that you can’t tell from looking at someone what their muscle depth will be.
Get your thigh ultrasounded if you’re worried
Don’t let your doctor fob you off. My specialist gave me one look when I asked for an ultrasound to find out my muscle depth and said, “You’ve got nothing to worry about.” as he pinched my thigh to find some non existent fat… I’m not joking. I only wish I was. I got this done privately at Amersham Hospital but this review should mean none of you have to go through that.
Most of all, I want all women who use an auto-injector to get checked. It takes minutes and will hopefully put your mind at rest. This review is well overdue in my opinion but it’s great news that it’s happening. I think what will happen afterwards will probably include guidelines for administering auto-injectors including a simple basic ultrasound test to determine which injector will work best. It may be that the area to inject may change or we might have a different place each! Now that would be confusing. Perhaps an ‘X’ marks the spot tattoo would help?
Everyone will be different, but the closer to the knee on my thigh gave a shorter distance to the muscle so for me, this would be a safer place to inject. This will depend also on where the best muscle is on your own thigh and could vary for other people.
So have you used your adrenaline? What did it feel like?
Did you get a rush of adrenaline? or feel not much at all?
How do you feel about this review? Getting yourself an ultrasound?
Further reading:
Anaphylaxis treatment: current barriers to adrenaline auto-injector use, T. T. Song1,*, M. Worm2 and P. Lieberman, Allergy journal.


Excellent advice, re the ultra sound, Ruth – will add a note to the blog and the articles on Foodsmatter.
Thanks Michelle. The review should help us understand more fully exactly what happens when you inject an adrenaline auto-injector and whether we should be taking more care to advise people WHERE to inject. Better to armed with the facts I always say.
A really interesting article Ruth!
Made me think outside the box. We become so reliant on things that we fail to consider the what ifs?
With my chunky thighs,I’m glad its my son that needs it and not me!
Thanks Alison, yes the men are all pretty much OK I reckon, they don’t tend to lay fat on their thighs do they? Hopefully the review will allay all our fears and mean everyone knows which injector will work for them and where to inject. Will be confusing though it that differs from person to person…
Hi Ruth,
Just wanted to add that although the needles on the Epipen and Jext are shorter than the Emerade, the adrenaline does come out with force which takes it much deeper than the needle length.
However I do think that girls who need to carry adrenaline should be aware of the issues and ensure they don’t get too chunky around the thigh area!
Hi Sue, I hope you’re right. I guess my experiences have made me wonder. And if the needle hasn’t pierced the fascia will the adrenalin even get into the muscle if the layer of fat is too thick? It does need to injected into muscle for the best results. Now I must get out for that run to keep my thighs in shape! Should they need a date with the needle, I want them to be at their best!
Indeed so Ruth, and Richard Pumphrey’s recent research seems to bear out your experience. http://www.jaci-inpractice.org/article/S2213-2198(14)00542-X/abstract
Perhaps we do need to worry about kids – “Dr. Arkwright from the University of Manchester used ultrasound to take skin surface to muscle depth measurements at set distances down the thigh and leg of 93 children. They also measured weight, height, waist circumference and body mass index (BMI).
At one quarter down the thigh, 82% of the obese children studied had skin surface to muscle depth greater than [Epipen] needle length. This was only true for 25% of the non-obese children.
Yet three quarters down the thigh, skin surface to muscle depth surpassed the length of the auto-injector needle in only 17% of obese children and 2% of those not obese.
“Based on our study, injecting epinephrine into the lower rather than upper thigh would be advised in overweight or obese children,” explained Dr. Arkwright. “If a child is experiencing anaphylaxis, this information would be important for a caregiver to know so that epinephrine can be administered into the child’s muscle in the most effective way.”
• This study was presented during the 2013 Annual Meeting of the American Academy of Allergy, Asthma & Immunology (AAAAI)
It is very worrying if even young kids could have issues with needle length. This study is very long overdue but at least we know now, if you are at all worried, administer lower on the thigh for more chance of success. You might expect obese children to be at risk but 25% if non-obese children is massive! Thanks for sharing.