




You might think I’m crazy, suggesting you go and get an ultrasound before requesting a repeat prescription of your adrenaline auto-injector but it’s very important for women to understand something about adrenaline injectors. They are not all the same. Some have shorter needles and some women’s thighs have more fat on them than others.
Imagine if you were carrying around an injector which would never and could never work. How would you feel? It’s not good enough to just know how to use it, practice how it works and make sure you always carry an in date pen if it’s completely useless.
Why am I talking about adrenaline auto injector needle length?
If you follow me on twitter you cannot have failed to notice the tsunami of tweets from the British Society for Allergy and Clinical Immunology (BSACI) conference which flowed while I was there. Search for #BSACI2015 and #BSACI. I learnt so much my brain is now full to bursting – look out for more blogs about what’s going on in the allergy and eczema world in the coming months.
The main reason for my attendance at the event was quite a serious one and a subject I feel very strongly about.
It’s nothing new either, which is why I am so angry because this could be a matter of life and death. If you are an adult woman who carries adrenaline or you have a daughter who does you should read this and act. If you have an EpiPen or Jext you should get an ultrasound soon, which I admit isn’t as easy as it should be but vital to determine whether the pen is suitable.
Needle length of adrenaline auto injectors is very important for women.
You can read about the adrenaline auto injector needle length debate here.
I spoke in a session organised by Bausch and Lomb who now own and manufacture the Emmerade auto injector. They held a special symposium about the needle length debate and asked me to speak which was both an honour, a privilege and terrifying all rolled into one.
Speaking at the symposium were:
- Richard Pumphrey – about whether the needle length of adrenaline auto injectors would deliver a dose correctly.
- Dr Rebecca Knibb on intuitiveness of adrenaline auto injectors.
- Ruth Holroyd – what it’s like to have anaphylaxis and discover your adrenaline might not be working.
My reasons for requesting an Emerade are very close to my heart, having used an EpiPen and Jext before I had never ever felt a rush of adrenaline. Not from the pens anyway.
After my most recent anaphylactic attack (thankfully over a year ago now) it suddenly hit me.
Was I really getting any adrenaline into my body at all?
Or was I just assuming that because I am still here that it must have worked?
I have always needed more adrenaline from the paramedics and have then felt much better fairly quickly.
I later read about the needle debate from Michelle Berriedale-Johhson on the Foods Matter website and alarm bells began to ring very loudly.
Speaking to my doctor wasn’t much use. He just pinched my skinny thigh and told me I had nothing to worry about… he also told me on another occasion that I couldn’t possibly be allergic to nuts AND dairy! What was I? Greedy or something? In allergy speak I’m positively obese with allergies, having anaphylaxis to all nuts, dairy and soya and less dangerous delayed but still allergic reactions to a myriad other foods and contact allergens.
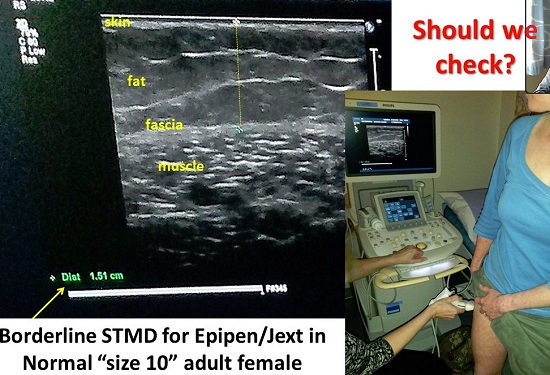
Well I pushed for an ultrasound, which I eventually got done privately at my local hospital; I went with a friend who also carries adrenaline for moral support. My thighs were shown as very borderline and when you add clothing to that, and the learnings from Richard Pumphrey’s study, I decided to play safe and get a pen with a longer needle. The jury is out as I haven’t needed to use this new pen yet… but I almost want to to see if I feel an instant rush of adrenaline.
When you study Richard Pumphrey’s findings there is definitely too much fat on my thighs for the normal 15mm needles to reach my muscle. Adrenaline must be delivered right into the muscle to be effective. Mine would have got to within a few mm of reaching the fascia so had I been carrying around a useless placebo all these years?
If nothing else the pens had given me peace of mind that I would have some line of defence should I have anaphylaxis. But that is not enough… when you know that your pen is useless, as mine was, you can’t just sit back and let others walk about with their placebo pens too.
How long till someone dies from anaphlaxis because the needle on their pen is too short? I don’t want to have that on my conscience.
If you are a doctor or prescribing chemist – can you honestly say you aren’t worried about this too?

Richard Pumphrey also showed that over 80% of women’s thighs had too much fat for a Jext or Epipen to be effective. This research was from a study looking at ultrasounds of women who were being prescribed adrenaline by Professor O’Hicky who ultrasounds all his women allergy patients. Thank you Professor Hickey!
What they have both proved is that BMI has nothing to do with it but being female most certainly does.
I’m fairly healthy size 10 (don’t put me to any tests, I haven’t been running for months) so my thighs are fairly lean. To look at me you might assume that any pen would work.
Not so, and not so for size 8 Poppy Harvey whose autopsy proved that her adrenaline injector had been ineffective at reaching the muscle. Could the right pen have saved her life?
Emerade is also much easier to use
The very lovely and beautiful Rebecca Knibb spoke second, about the ease of use of all the pens on the market. Emerade came out tops here too for intuitiveness and simplicity.
I can’t sit on my hands and not share this with you all again. I have written about it before but I have to start shouting.
If you are female and carry adrenaline please get your leg ultra-sounded to check you have the right pen and get am Emerade if you need one.
I am hoping that our message did get across at the BSACI. The room was packed with hundreds of people and standing room at the back so I do know what adrenaline feels like. I was shaking with fear and the adrenaline pumping around my body preparing me to run from that stage and escape was immense. It was a great experience though and probably my toughest speaking engagement yet and really experienced audience.
So my question to you today. All you women and daughters and aunties and friends. Are you doing to ignore this blog post or encourage your allergic friend, mother, daughter etc. to get checked out to make sure they pen will actually give them a fighting chance to beat anaphylaxis.
If you’re a doctor – what will you do next time you prescribe an adrenaline auto-injector?
Get an Emerade pen and get your thigh ultrasounded
All women should have an Emerade pen which has a longer needle which is 25mm compared to Jext and EpiPen which have a 15mm needle. If you can’t get an ultrasound or don’t want to pay, just request an Emerade pen today to be on the safe side. However some people may not even be suitable for an Emerade so if you are worried do get an ultrasound – it’s better to know and carry a surgical needle and adrenaline to inject. Even if you are too scared to inject a proper needle which needs the drug drawing into it and injecting correctly, at least you’ll have the proper drugs on you when you need them a paramedic or doctor could administer.
References
The BSACI also hosts hundreds of posters which showcase various studies in the area of allergy and immunology. The Stevenage poster is also really important as it highlighted that children prescribed Epipen or Jext (irrespective of gender, weight/BMI or height), have only a 50:50 chance of getting an IM injection. The Worcester paper showed that only 1 in 10 adult women will get an IM dose….so this is all really worrying.
Rebecca Knibb – testing the intuitiveness and ease of use for adrenaline auto-injectors.
The deep fascia of the thigh forms an impenetrable barrier to fluid injected subcutaneously by autoinjectors. Pumphrey et al 2015

So if the pen isnt going to work if I stick it in your thigh…..where is best??
I hope and pray I never need to know to do this…for you or for anyone else, but I might…you never know….Knowing how and why..might just save someone….
It’s a tricky question, if they don’t have an Emerade the advice is that closer to the knee would mean less fat. If you look at where we are advised to inject, it’s right smack bang into the fatty thigh tissue, but you also need muscle mass below the fat so it can’t be too close to the knee. Maybe we should get a tattoo – you know, X marks the spot. Inject me here! after ultrasound is done to confirm the sweet spot. For some women and obese men even an Emerade may not have a long enough needle and for those individuals they would need a surgical needle and phial of adrenaline and training how to use it. I’m glad I don’t have to do that. I hope this helps but am going to go and ask some medical friends now what they would say to do in a case where you are nor sure where to inject in an emergency.
Advice is possible calf? but front of thigh better than side of thigh if in doubt but yes, hopefully you will never need to really use one in an emergency.
So which has the longest needle and shouldn’t we just request that one? And how much did your private ultrasound cost? Many Thanks
Hi Natasha, yes you should most definitely go and request an Emerade pen which has a much longer needle. I can’t see why your doctor wouldn’t prescribe it. I’ve had one for some time now so it was last year when I requested one. It was a while ago re the ultrasound too but it wasn’t cheap. I think it cost £30-40 but I don’t think you should have to pay, I think this should be on the NHS. Get your doctor to read this and ask for an ultrasound. It takes minutes to do and isn’t an expensive procedure.
Hi there
I have been reading your blogs with great interest. I took an allergic reation to cucumber last night and had to use my epipen. I was definately going into anaphylaxis, my partner called 999 and they arrived thankfully in about 6 mins. I didn’t have much relief from my dose and reading this, it maybe due to having very thick thighs. The emt administered the adrenaline in my arm, I felt better about 10 mins later and was taken to hospital, given iv steroids, and after a period of observation, let home. The reason I ha e an epipen is I took a similar reaction last year to watermelon, may iadd, both of these products were pre-packaged snack packs. Could this be a factor? I’m waiting on my gp surgery opening to ask for further tests. However I’m now frightened to eat anything in case I relapse. Its horrendous. Should I be injecting an epipen into my arm? Is this suggested if thighs are too fatty? I will ask for the emerade pen though. Also I have eaten both these fruits all my life without issue. Why now? Any help would be appreciated, I’ll also do more reading so I’m well armed going to my gp, if I ever see one these days.
Kind regards
Rosslyn Robinson
It’s a little worrying I know and I don’t think the Emerade pen is available any more. What I do is remember that I can inject a little closer to the knee, into the muscle still but it should have more chance of getting through the fascia into the muscle.